Excel symptomdiary userguide
Version 2007/E1
PERMISSION:
Patients suffering from chronic
illness(es) have my permission to download the MASTER Excel symptom diary and userguide from http://LymeRICK.net - and may modify, save
and use their own
personalized version and
may use this tool for FREE - in order to help create better overview and keep
track of course of a very complex long term disease symptomatology.
COPYRIGHT:
The diary was created and is copyright by Marie Kroun, MD - Denmark. Email: kroun@ulmar.dk
My
name, copyright notice and email address must NOT be removed from the diary and the MASTER TEMPLATE may not be altered
in any way by others than myself, and may not be
distributed
via other websites / media than http://LymeRICK.net - this of course to ensure
that there
is ONLY ONE VERSION - the latest update - of the diary available on
the Internet.
Don't try to correct the calculations or the curve drawings
yourself, because this could lead to unexpected errors; you should
always report found errors and suggest
improvements to me personally -
I'll then correct and update the MASTER DIARY on the
LymeRICK website
ASAP.
DISCLAIMER:
The symptomdiary was developed in a
danish Microsoft Excel version 2003 with help from project
participant, that were all highly suspect of / or proven (positive
antigen test) to be suffering from tickborne infection(s), mainly
borreliosis; but the diary would be useful to help evaluate and follow up on the course of any chronic illness.
The danish version
has been in
use
for
5 years and no errors have been found in the last year
before
translation into English. However, I do not guarantee it will work on
your computer, i.e. when the diary used in other language versions of
Excel? - in DK
we use COMMA
(,) as decimal delimiter, and date form is DD-MM-YYYY (short DD-MM-YY),
if you use other formats, it might create problems? - I have
not
been able to test the translated
version of the danish diary in english versions of
Excel - please try it
and report back to me how it works, especially if you experience any
errors. Suggestions for improvement are very wellcome, likewise should you find any errors,
or if you need help with evaluation of your personal diary, feel free
to contact me.
BUT NEVER SEND YOUR DIARY TO ME AS EMAIL ATTACHMENT;
always write me an email first and present yourself,
then I'll give you a personal upload area on my
webserver to upload the diary!
Make sure you have downloaded and use the latest
version of the diary from LymeRICK, otherwise
I will not spend time to help find and
correct eventual errors reported!
Introduction:
The idea of using a symptomdiary is far from new in medicine,
but most doctors just ask their headache patient to make notes on
headache attacks only and asthma patients to do peak flow metry in
order to follow course, but with this diary you can follow ANY SET OF
SYMPTOMS and analyze them.
Using a score system is not new either.
Many have used a VISUAL ANALOG SCALE
- usually grading symptoms from 0-10 - in order to try to MAKE SYMPTOMS
MEASURABLE AND COMPARABLE OVER TIME
- both in the
individual patient during course of
his/her illness, and/or when comparing
different patients, when the doctor pool data from
several patients and find common features of a particular
"disease
pattern".
However, without putting EXPLANATIONS IN WORDS to what a
particular SYMPTOM SCORE means exactly, we risk
that psychological factors may influence the score much, depending
on
the patients mood that day i.e. "same symptom grade" may be
scored more variable over time and the perception of a
particular score number may differ
quite much from patient to patient and among patients and doctors,
depending on what they have had of previous experiences, grade of
tolerance to pain etc. etc.
No patient - that spontaneously chose
to use the 10
point visual analog score system in the beginning - could ever tell me in clear words
when they gave 7 respectively 8 points - therefore I could not
be
sure they would use the score consistent over time for same grade of
a certain symptom.
After letting project patients chose and test different score
systems and gaining experience from that - I decided to steamline and use a simpler scale with
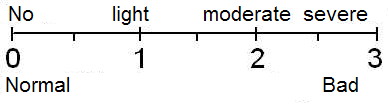
fewer numbers, the severity of each integer grade values were explained by words, as follows:
0= normal; normal function, should NOT be written into
the diary; empty cells automatically count as ZERO!
1=
slighly abnormal (reduced function)
2= moderately abnormal (function
difficult)
3= severely abnormal (worst ever, function impossible)
and >3 can be given IF a patient later should worsen
above what (s)he thought possible / have experienced before!
In this simpler visiual analog scale, it becomes possible to explain grades / symptoms in
plain words, which we humans can usually relate to much better,
than
we can to numbers.
OVERALL SEVERITY / function loss can then be calculated by
dividing the peak and the basic symptom score level respectively by 3
i.e. number of symptoms scoring highest niveau, where function is
impossible!
However it soon turned out that the "sensibility" of the above 0-3 score system was reduced if
all symptoms - 1/2 or 3/4 in between two integer
scores - are rounded down to nearest integer value all the time; then minor symptom fluctuations may be cut-away from the curves,
especially
when a patient has few swinging symptoms and many relatively stabile
high symptoms, which is quite often the case in long term illness.
Thus if 0,5 points is removed from say 10 symptoms each, this would
give a reduction of total 5 point on the total symptom score,
i.e. 10% missing points on the total score if the patient has a high
basic total score
level about 50 points - which again corresponds to maximum score
(= patient is unable
to function because of the symptom) for as many as 16 symptoms - this is clearly a very disabling
condition - the patient need help!
Both the simplicity of the 0-3 point scale and sensitivity can both be easily achieved, however, by asking the patient to score his/her symptoms in DECIMAL VALUES - illustrated in the ruler below:
Judging the diary:
Because computers / the Excel spreadsheet can calculate / sum up NUMERIC SCORES and draw curves for us
- per symptom, per organsystem, and total plus treatment curves
- all made automatically and instantaneouly, along as the patient enters the scores ... we
can create overview over a complex
multi-symptomatology, evaluate for potential symptom triggers, as well
as keep a close eye on the course of disease over long
period
of time, perhaps during a trial treatment, as well as register adverse effect; when the diary has
been kept for a while (at least 1 month in chronic illness)
before,
and later during
and a suitable period (at least 3 months) after a trial intervention,
the result
of
this intervention can be easily judged on the curves and analyzed in
details: declining scores means improvement, increasing
scores means worsening (side effects > beneficial
effect) and no change / lag phase, means there was no effect; logically a harmful
or ineffective treatment should be stopped, when we've seen it does
not help the patient!
Fluctuating symptoms points us to either cyclical infectious
acticity or to repeated exposure at timely intervals to other
environmental toxins / allergens that cause "infection like" symptoms.
The cycle may tell which infection(s) could play a role in the disease
picture, if typical / known growth pattern from laboratory science or
previous clinical experience!
Persistent, non-fluctuating symptoms can be due to either permanent tissue damage,
accumulated toxins and/or accumulated degradation products - or
probably a combination of the three.
Active infections often produce toxins and degradation products
that trigger immune reaction; even after active infection - and
hence further microbial toxin production - has been gunned
down by relevant causal treatment (antibiotic), it can happen, that
excretion
of toxins and degradation products (healing) can be very slow
and insufficient, possibly because of a bottle-neck situation
in the detoxification system
- then excess toxins can't be excreted (in between symptom
flares),
but tend to accumulate over time and may cause gradual worsening,
because when not eliminated, continue to trigger all the
proinflammatory immune
reactions, i.e. will give
the patient continuing symptoms on a relatively high basic level after
infection (post-infectious symptoms)
Only ACTIVE MICROBES - when sensitive - can be gunned down by
antibiotic treatment.
CHRONIC ILLNESS - (neuro-) toxin mediated? - symptoms may not occur
until "the cup" has been filled and the detoxification system is being
overwhelmed. It is a simple matter of balance between input and output.
The more toxic stuff (including microbial toxins) the system have accumulated over time and
need to degradate and excrete via the same metabolic pathway, the more likely a bottle-neck situation
can occur, when further - microbial - toxins begin to pile up on
top, and when the treshold become exceeded, symptoms are
produced. When severe, the patient may suffer from multiple chemical sensitivity
symptoms (MCS), where just a tiny bit more will results in very severe symptom
aggravation. In these cases it is pertinent that the patient - and only (s)he can do
it! - cleans out all unnecessary things and only take in healthy foods;
many medicines have to go through the same pathway too and severe
adverse effects can be expected in the MCS patient; to reduce worsening
reaction start with very low dose, and increase very slow and not until
an eventual induced adverse reaction have cleared!
Excretion of some toxins can be increased by toxin binders; I refer you
to read Ritchie Shoemakers books and website for further nformation on this
subject: http://www.chronicneurotoxins.com
In borreliosis, we have unfortunately no way to tell the
difference between
a true cure
(eradication of all borrelia from the host's body) or latent stage (dormant,
inactive bugs that might later have a chance to grow up again).
Therefore we will
need to keep an eye on the basic symptom level for a long time after
stopping antibiotic treatment!
According to dr. Burrascano there is a very good
chance that a patient that has not had relapsed within 3 years after
stopping antibiotic treatment, will not relapse later - i.e. the
follow-up time should be at least 3-5 years (like most cancer
patients); on the other hand treatment should probably continue
for as long as it seem to be of benefit to the
patient, i.e. as long as the patient continues to improve and there is
still sign of activity flares, judged by falling basic symptom level
and repeated peaks, usually at monthly intervals.
In the diary
we can evaluate which symptoms swing (together) and which don't - i.e.
which symptoms represent flare activity, from which we may
guess
on a particular infection.
The flare pattern can say us something about which infection(s) could
be in play (which should we use money to test for?) because some
microbes have a cyclical growth pattern giving the patient a
cyclical symptom pattern - just to mention a non-tick vektor borne
infection: malaria, this infection is also named "tertiary fever" because the relapses
comes at 3-4 days interval ... borrelia have a "quick" cycle of
about 9 days interval (like in relapsing fever borreliosis) and a slow
cycle of 3-4 weeks interval, probably dependent on how long time they
have been dormant before reverting to activity (Brorson).
Likewise malaria cycle with infectious disease symptoms every 3-4 days,
and the ringforms found in RBC of my project participants seem to flare
at about 4-5 days intervals ...
The symptom list and grades:
The long symptom list came about, by adding all symptoms project patients registered, some used dr.
Burrascano's list (see his guidelines at http://ilads.org
) and I added some symptoms / triggers too, plus MEASURES like temperature and pulse, which are important
infectious markers, that must be followed at least a month to judge if
there are fluctuations like in "relapsing fever borreliosis" that
gave fever (plus general malaise symptoms, chills
& sweats) in attacks
at about 9 days intervals!- and some measures the doctor may
do in the clinic - and some known possible triggers of symptoms.
Then all
"pieces of the puzzle" can be
evaluated together and make it easier to notice what is common features
of the "disease picture" under investigation.
Most import, all symptoms,
the course of disease over time, plus effect
(wanted as well as side effects) of treatment trials becomes VERY WELL
DOCUMENTED and not forgotten.
We can always compare later events to previous events, when we have
saved the diary!
The degree of disability can be read directly from the total
symptom score! - total score / 3 = number of symptoms that are so
severe that the patient is unable to function!
The many symptoms you CAN score in the diary may overwhelm you at first
glance - but don't despair - because YOU NEED ONLY PUT SCORES IN FOR SYMPTOMS
THAT
YOU HAVE - i.e., symptoms which are ABNORMAL, i.e. ABOVE ZERO.
Except for temperature and pulse
(potential flare markers, when you suspect that a CHRONIC
INFECTION cause your symptoms), and at least one
height and weigth (necessary to
calculate sufficient dose of drugs)-
YOU
DON'T have to measure everything
every day, nor continue measuring it all for years, just do it long time
enough to be able to spot the "basic level" before eventual
intervention (1-3 months) and if there is a regular flare activity
pattern, which of course depends on the type of disease.
IF your temperature measures are lying
stabile within normal range for
about a month and do not show any visible flareswings, you can stop the
daily measures and only do controls, if
you later feel abnormal / changed.
But - because we need to take eventual cyclicity
into consideration, when chosing the best time for drawing blood for
ANTIGEN TEST, you should not stop the diary until you have a
plan
for testing / permission to stop the diary from your doctor!
The slower the growth velocity of microbes the longer
observations time is needed to judge both spontaneous untreated course and result of treatment!
Sometimes exposures to environmental toxins (molds) or toxins
in food
or known allergens can elicit an immune reaction and may even cause
a FEVER and thereby imitate an INFECTION.
Therefore I added some of the more common exposures to known
toxins, including some that some
people use out of free will as stimulants, like tobacco, coffee and
alcohol! - that may cause or aggravate some of the symptoms - in that
case you
should abstain from continuing the use of the suspected trigger, at
least
for a while, and then read the result of the pause, on the symptom
score!
You may add extra triggers, when you suspect
they could have influence on some of your symptoms!
I tried my best to make the symptomscore chart easily
adjustable to accomodate to individual
needs and to become usable for all sort of chronic conditions
/ following
any treatment trial, whether conventional or alternative. However if
you add something, calculation and curves also need to be added
manually, if to be shown on curves too - this is not a "do-it-yourself"
matter as described above, unless you are very familiar with Excel!
IMPORTANT NOTES before you
begin registering your symptom scores:
- Print out the user guide ONCE and for all, so you can
always look up the explanation in words for the indiviual integer
symptoms scores.
- Microsoft Internet Explorer may seem to let you enter data
into
the spreadsheat after opening it on the LymeRICK website, but you can
only save the by you altered spreadsheet on your own computer, you are
NOT ALLOWED TO OVERWRITE the MASTER TEMPLATE on the LymeRICK
website, of course!
- After downloading the template from my
website, you must start with entering all your personal data
and facts about your
previous disease history in "PERSONAL DATA" and the "PRE-DIARY
STATUS".
- In "SYMPTOMSCORES" you must add
all your current
medication, nutritionals, additional symptoms / possible triggers to
keep an eye on.
- SAVE YOUR
PERSONALIZED TEMPLATE WITHOUT ANY SYMPTOM DATA IN!
From this PERSONAL TEMPLATE you can PRINT an empty paper
diary out (for 7 days, 3 pages)! - papers
can be taken with you when you're not at home, can
be filled out
while you are lying in bed, or by help from your family, if you are
unable do it yourself! - and
the data can always be entered into the computer later! -
by you or family / friends, if you are unable to do it yourself!
- From your personal template, save a
working copy under your-name+startdate+enddate.
Enter dates in filenames in the backward format
YYYYMMDD,
then the symptom diary files will be automatically sorted in
timely order in your directory, this gives good overview over versions!
- Take BACKUPs
of both your personal
template and of your continuing Excel symptom diary on
different
storage media (like a memory stick),
so you don't risk losing your important data
forever, in case your Excel file or harddisk suddenly becomes
corrupt :(
Always keep
last weeks copy for safety in case you make error when entering
data; you can then reload and start all over; when 6
months diary period is
completed, save this file forever on multiple media (you should also
write protect your finished 6 months diaries for safety) and
print out curves for you paper copy to show your doctor the course :)
IMPORTANT NOTES when filling data into the SYMPTOMSCORES spreadsheet:
- SUM SCORES and
CURVE DRAWING can only be done on NUMBERS,
therefore never
enter TEXT (literals) within in the calculation are,
i.e. only text in COLUMN A!
- Entering the wrong DECIMAL DELIMITER may cause
error?
- if curves are not drawn as
expected, it could be because you've enter 1.75 instead of 1,75
(the
diary was made with a Danish Excel 2003 version), using the wrong delimiter
turns the number into a text string!
- DATE - the form must be enteres as DD-MM-YYYY or / short DD-MM-YY.
X-axis (the time line) on the curves are
automatically picked from
the first DATE (column B, row 3 = cell B3) and until the next
empty date occurs
- therefore DO NOT LEAVE
ANY EMPTY HOLES IN THE DATE ROW!
Entering a wrong date (typing wrong year is a very common
error,
especially after New Year) will corrupt curvedrawing, because
X-axis will adjust according to all the dates entered (try it and see
what happens).
You can use the automatic filling function in the DATE FIELDS,
by pulling the little
dot in the lower, right corner of the date field with the mouse; then
you
can quickly and easily add more dates, without risk
such typing errors.
If the start and/or end date(s) of your curves is
outsite the
period you have registered symptoms for, you must have entered
a
wrong date
in some place, find and correct the error!
The curves are stretched to fill the whole width
of the curve chart, thus the
more dates entered, the more compressed the curves will become over
time.
- You should shift spreadsheed after 6 months, there are vertical lines per month. I've
made some statistic calculations per months below
the calculated
total scores (min, max and mean scores per 31 days periods)
Check on LymeRICK first if there is an update of the MASTER
version, if yes download and transfer your personal data to it and save
as new template; otherwise base the new diary on the last you
filled, just save as new startdate and clear all the data and dates.
- MEASURES should
always be done under "basic / comparable conditions",
i.e. after at
least 30 minutes rest, same time of day (extra measures per day can be
added under your PT notes, just remember to add time of sampling too);
temperature should be measured in rectum preferably, if in mouth:
no warm or cold intake for
10 minutes before and measure with closed mouth; Blood pressure: always
either in sitting or in lying position and on the same arm (the arm
showing highest blood pressure)! - always use same apparatus for the
measure;
Results
of measures are entered exactly as the apparatus show,
i.e. do not add anything for measuring temperature in your mouth or ear
- which is normally a bit lower than
in rectum - instead make a note in PT-notes on how you measure
temperature, once
and for all, then the doctor will know how to judge the
measure!
ENTERING PRESCIPTION DRUGS / REGISTERED NATURAL
DRUGS:
In your personalized version in SYMPTOMSCORES columna A, you enter all
drug names, the prescribed dose (mg/tbl, mg/ml) and number of times per
day
to take the doses:
ex: T. metronidazole 500mg x 2
or bricanyl mixture 0,3
mg/ml, 5 ml (1,5 mg) x 3.
UNDER THE DATE SUM UP ALL DOSES TAKEN THAT
PARTICULAR DAY without text! - if you add "mg" after the
number, curve will not be drawn!
ex. metronidazol: 1000 (~ 500*2)
or bricanyl mixtur: 4,5 (~
1,5*3)
Supplementary treatment is entered likewise as for
presciption drug, when
possible! - it is VERY IMPORTANT TO REPORT
EVERYTHING TAKEN, also non-prescription drugs like
painkillers ....
If the
immune function is reduced due to toxic reaction and/or detoxification
is generally hampered by lack of essential nutrients (vitamins and
minerals are important co-enzymes, lack of which may reduce / block
enzyme function => bottle neck in the detoxification pathway),
then
we can expect worse side effects and may need to START
WITH REDUCED DOSE and SLOW INCREASE after any reaction has
passed, in order to avoid too fierce worsening reaction!
You should have scientific data present about all
alternative drugs that you use and give your doctor a copy, because
some natural herbs may actually interfere with metabolism
of prescription drugs (increase or slow detoxification) or may cause
known side effect / bad interactions with other drugs that you take,
that could perhaps explain some of your symptoms.
There are many possible alternative treatments it could be interesting
to register
IF there is positive effect of: physiotherapy, massage, chiropractic,
zone therapy, physical
training (note what, duration and grade in PT-notes) etc.
etc.!
NEVER START A NEW
SUPPLEMENT / TREATMENT without first discussing with your doctor,
if it interferes with other things you take and may give unwanted
adverse effect.
When a patient is multi-medicated, is becomes
very difficult to judge which effect / adverse effect comes from which
single / combination of preparation(s).
Trial treatments should be planned in such a
way, that we
are able to read the effect from that intervention specifically in the symptom
diary - i.e. preferably keep everything else un-changed!
A "spontaneous" improvement can occur when a bug goes into latent stage
without any known reason, or could perhaps be result of a lifestyle
change the patient made; we'll need several patients - that
are
comparable in duration of disease, severity, known causes, age, sex
etc. etc. - that try the exact same intervention, in
order
to compare results / pool data and find out if an improvement
was most likely coincidental (few react the same way) or if it could be
a treatment effect (most react the same way).
When using the diary before during and after an intervention, the
patient can act as his/her own control for example by cross-over - i.e.
a
period without treatment / exposure to trigger can be compared to
a period on treatment / exposure to trigger and again another
period without / without treatment / exposure to trigger.
If the reaction is consistent on/off several times, we probably see the
result of the intervention.
NOTE do not make these shifts in intervention without discussing it and plan it all with your doctor;
some drugs need pretty long time to show full effect, and some drugs
show adverse effects in the beginning that may reduce along as the
detoxification system adjust enzyme level to clear the drug (tolerance
development); some drugs may create dependence, i.e. the patient can
get withdrawal symptoms; in such cases the intervention must be
gradually induced or retracted.
SUGGESTED SCORE SYSTEM:
(you can change description if you need to! - but then you can't compare with
other patients scores and your doctor can not compare your data with
others, make it more difficult to judge your situation!)
NOTE 0: NORMAL CONDITION may be explained in []
DON'T WRITE
ZEROs
(normal condition) INTO the SYMPTOMSCORES, only scores >0. ZERO is automatically assumned, when a cell is left empty!]
Toxin / allergy / diet-break EXPOSURES must be noted:
Explain in
PT-notes what, when, how long, how much, and describe you reaction with
words.
ALLERGY-like reaction:
1: non-characteristic, but reproducible reaction after contact with the
toxin / allergen
2: localized hives / excema without breathing difficulty (asthma) or
circulatory disturbance
3: generalized hives or severe excema, and/or asthma and/or circulatory
disturbance (shock)
ALCOHOL-intolerance:
1: slightly sensitive; a single glass of beer or wine is tolerated, but
reaction to less than usual for you (explain how much you usually
tolerate).
2: moderately sensitive: feels intoxicated after a little cider or a
low-alcohol beer
3: very sensitive; no alcohol tolerance, you can even feel sick /
intoxicated after smelling alcohol or perfume (~multiple chemical
sensitivity)
General wellbeing/malaise, other symptoms not related
to specific organ systems, functions
Swollen glands:
- describe in PT-note which glands are swollen and size
[0 = no]
1 = yes
Chills- and sweats - feeling cold (may be important infectious symptom
flare markers)
- during a flare, please measure temperatures several times that day at 2-4 hour
intervals,
because sometime temperature changes may occur quickly as fall/rise during 6-12
hours!
1: cold without sweats or warm without chills
2: chills, feeling cold, need more clothes on to get warm,
than
other people in the same environment OR feeling hot, but not
with
drenching sweats
3: very cold and feeling multiple chills after another, cold hands and
feet; have to take a warm bath/ sauna and go to bed with clothes on to
warm up, later break out in drenching sweats
Colour of skin (paleness / redness)
1: short attacks of redness or paleness
2: redness / paleness of longer duration (noticed by others),
3: very pale / gray / bluish tint OR red flushing tint (perhaps as
Harlequin phenomenon (one-sided))
Fatigue:
1: a little tired, clears after a short pause / rest
2: moderately tired, need to rest/sleep one or more times during day
time
3: extremly tired / exhausted, need to rest all the time during day time
Disturbed sleep pattern:
[0: normal (at least 6 hours sleep in a row during the night)]
1: sleeping less than (<) 6 hour in the night, but is relatively
rested in the morning - need to have a nap in the afternoon
2: sleeping only short time in a row, turning around night and day, not
rested in the morning despite min. 8 hours sleep per 24 hours
3: sleep only minutes at a time, don't sleep at all or sleeps more than
(>) 12 hours per 24 hours.
Menstruation:
0,1-0,9: Spot-bleeding
1: normal menstruation
2: bleeding more than normal
3: excessive bleeding
Perimenopausal females only:
Actual number of heat waves per day (short duration i.e. seconds to a few minutes)
Mobility:
[0: normal = no appliances needed, walking distance 500+
meters]
1: using a cane or walking distance in range 100-500 meter
2: using a rollator or walking distance less than 100 meter
3: using a wheelchair / bedresting / walking distance 0 meter
Need of nursing:
[0: no need for help]
1: need help with domestic work, cleaning etc. - describe in notes what
you need help with and what you can do yourself
2: need a little help with personal care
3: need extensive help with everything
Eyes:
(if problems: write Right / Left in PT notes and do Functional Acuity
Contrast Test (FACT) or VCS at http://chronicneurotoxins.com
)
Light sensible:
1: slight, but no need for sunglasses
2: moderate, uses sunglasses in clouded weather and indoor
3: severe, can't stand light at all, must wear very black (noir)
sunglasses / mask
Blurred vision:
1: slight, letters blurred but can read
2: moderate, letters more blurred, difficult to read
3: severe, everything grey in grey, can't read letters
Double vision:
[0: no]
1: yes
Night vision: (check for A-vitamin
deficiency)
1: slightly decreased discrimination, tiring to drive car in twilight and dark
2: moderately decreased, can't read roadsigns in twilight / dark
3: severely decreased, everything blurred, unsafe to drive car
Estimation of / ability to judge distance:
[0: good, normal]
1: bad, difficult
Floaters ("mouches volantes") inside the eye:
1: a few
2: a lot
3: many
Red eyes, secretions, pain (conjunctivitis):
1: slight irritation, no redness
2: moderate irritation, slight dry secretion, slightly red conjunctival
vessels
3: severe irritation, pus, very red (bloodshot) eyes, pains
Ears, sinus cavities:
(if problems: write Right / Left in PT-notes)
Hearing:
1: slightly decreased
2: moderately decreased, hardness of hearing, difficult to understand
speech
3: deaf
Sound sensible:
1: slightly sensible, no difficulty hearing talk
2: moderately sensitive, have trouble hearing what others say,
when in a room with much noise, like when many people talk at the same
time or TV/radio is turned on
3: severe, can't stand noise / talk, have to wear earplugs
Tinnitus:
- describe character of the sound in PT-notes
1: short tones (lasting seconds to minutes)
2: tone lasts over 1 hour
3: tone constant, allways present
Ear pain:
1: slight - painkillers can remove the pain
2: moderate - only slight effect of painkillers
3: severe - painkillers don't help at all
Tuba occlusion / like having an earplug closing the auditory canal:
[0: no]
1: yes
Nose, discharge, airway passage:
[0: normal, free airway in both nostrils]
1: slightly swollen mucous membranes, but airway passage - if
discharge/snot, describe looks of it (clear/yellow muddy,
thin/thick, +/- blood)
2: moderately swollen mucous membranes, passage closed fully in one
nostril at a time, partial passage in the other
3: both nostrils closed for air passage all the time, breathe through
open mouth
Sense of smell / olfactory sense:
1: slightly reduced
2: moderately reduced
3: severely reduced, no sense of smell
Chest area, heart, lungs:
[ PULSE = number of heartbeats per minute must be
entered
under measures (Normal range 60-80; over 100 tachycardia, below 50
bradycardia) ]
Number of attacks of irregular heart beats
Number of missed heart beats/block:
1: slightly abnormal; a few missed beats, duration less than 5 sec. -
write in PT-notes if extrasystole was seen on ECG
2: moderately abnormal; pulse 40-60, or pulse stop for 5-15 sec.
3: severely abnormal (dangerous, life-threathening); pulse under 40 or
pulse stops for more than 15 sec (need pacemaker)
Minimal duration of heart arrhytmia (minutes)
Maximal duration of heart arrhytmia (minutes)
Chestpain:
1: slight - short stings / shooting pains
2: moderate, feeling of oppression / weight on the
chest, difficulty taking a deep breath due to pains
3: severe pain in heart / angina
pectoris
Cough:
- note describe dry or wet in PT notes
1: slight - a dry irritative cough, sometimes, write number of attacks per day
in PT notes
2: moderate - wet cough, about every hour, slight clear expectoration
3: severe - wet cough several times per hour, a lot of think slime or
suppurative mucous
Breathing difficulty / short of breath:
[0: normal, speaking effortless even when walking fast / running]
1: slightly short of breath after physical activity, but can speak
2: moderately out of breath, can not speak while walking slowly
3: severely breathless /dyspnoeic, gasping for breath, wheezing,
difficult to speak even when not moving
Respiratory pains:
1: slight, only shooting pains on deep breath or special movements
(nerve pain)
2: moderate, pains at every breath
3: severe, dare hardly breathe because of the pains
Oedema/Edema:
1: slight, deklive (foot and ankle, fingerpressure (shin) less
than 1 cm deep)
2: moderate, deklive ex. to middle of shin (evening), maybe
also eyes, fingers (morning), finger pressure
(shin) 1-2 cm
deep
3: severe oedema, deklive to knee or above in the evening, eyes and
fingers (and scrotum) still swollen part of or whole day,
finger
pressure (shin) more than 2 cm dybt
Mouth, Stomach, Intestine:
Sore throat/pharyngitis:
1: slight - stinging / irritation irritation, but not nedness
nor coating
2: moderate - pain when swallowing, redness, but not coating
3: severe - pain when swallowing, very red and coated mucous membranes
(describe in PT-notes)
Sense of taste:
1: food tastes a little diferent / or reduced
2: metal-taste, food much different
3: rotten or metallic taste all the time
Blisters, aptheae in mouth or throat:
1: a few (1-2)
2: a lot (3-10)
3: many (more than 10)
Nausea:
1: slight - can eat, relieves nausea a bit
2: moderate - eating difficult, doesn't relieve the nausea
3: severe - can't eat, results in vomiting when trying
Vomiting:
number of times per 24 hours
Bloating, belly aches, abdominal cramps, heartburn:
1: slight bloating, abd. pains occurring less than 10 times
per 24 hours
2: moderate (visible) bloating/distension, loud bowel noises
(borborygmi), abd. cramps more then 10 times, but not every hour
3: severely inflated, loud bowel noises with crisp, tingling
sounds, cramps severel times per hour
Defecations:
number of times per 24 hours
Stool consistency:
[0: wellformed]
1: hard
2: very soft and bulky (porridge like)
3: watery
Stool incontinence:
number of incontinence episodes per 24 hours
Appetite:
1: increased, eat more than normal (bulimia)
2: decreased, eat less than normal / needed (slight anoxexia)
3: no appetite, eating difficult (severe anorexia)
Urinary tract:
Irritable bladder / pain::
1: slight urge - bladder / urethral irritation / burning, need
for frequent urination, but can control it
2: moderate urge
-burning/stinging painful urination, must pee all the
time despite little urine to pass, can't control it
3: severe urge - bladder cramps/very painful, burning
urge plus urinal discharge, bloody urine
Urinations during daytime (06-24):
number of urinations
Urinations during nighttime (24-06):
number of urinations
NOTE if abnormality in frequency of urination and/or in
amount excreted (normal average is 1500 ml urine per day) we must have
details about what/when (3 days):
measure both your fluid intake (milliliter
& time), and amount & time per urination;
after 24 hours; calculate sum of intake
(excessive (~ (psychogenic?) diabetes insipidus) if intake is in range
6-10 liters per day) respectively sum of excretion and compare
since we use some water for metabolism and lose
some through sweat (more in warm weather and fever) excretion should be
less than intake of fluids.
MANY POSSIBLE CAUSES OF INCREASED URINE PRODUCTION:
* a very low intake of fluid (less than 1
liter/die) respectively * excessive drinking (polydipsia >3-4
liter/die) will influence the amount of urine produced; excess
is excreted;
* increased glomerular filtration rate occurs
during fever and hyperthyoidism; * decreased reabsorption of water in
distale tubule (kidney damage)
* diabetes insipidus: lack of
antidiuretic hormone (ADH, vasopressin) a pituitary hormone that
normally peak during night time, cause kidney to concentrate the urine
(so sleep is not disturbed),
hence damage to the pituitary (tumor,
inflammation, toxins) can cause lack of ADH and result in
frequent, large urinations, because urine can not be concentrated
without ADH
=> loss of water causes thirst;
Addis thirst test, urine excretion stay on same high level despite
fluid intake is reduced / paused totally; urine osmolarity do not
increase as normal during thirst
* increased excretion of solutes will draw water
out: salts, loss of albumine though kidney (due to damage to
glomeruli) or high sugar (diabetes mellitus) in urine and diuretics can
cause increased urination
* some herbs and alcohol also increases urinary
excretion!
Urine colour / cloudyness:
[0: clear, light yellow]
1: slighly unclear
2: cloudy, colour abnormal
3: bloody / very cloudy (can't see through it)
- whenever urine looks abnormal, describe how it looks, and if is
smells?
There are numerous causes of abnormal coloration of
urine, food and drug can affect it very much!
- urate and other salt crystal can precipitate in
concentrated urine can result in cloudy urine or stone formation (do
you drink enough?)
If urine darkens when left in the bottle over time plus patient has
abdominal pain, nerve pains and skin problems
(photosensitivity, blisters) - then suspect porphyria?
- porphyria can be intermittent and attacks can be provoked by many
triggers, among which are infection / drugs (certain antibiotics)
...
Urine incontinence:
number of leaks per 24 hours
Musles, joints, bones:
- decribe where and how in PT-notes
Neck & Back:
1: slight pain, non-irradiating, slight stiffness
2: moderate pain,
moderat stiffness, creaks and cracks
3: severe pain, movement reduced or locked /
pinched nerve / fact syndrom like / lumbago
Joints:
1: slight pain, no objective changes
2: moderate pain, slight swelling (may be due to peri-oedema) revert to
fully normal in silent phase
3: severe pains, redness and warmness over affected
joint(s), fluid in joint, synovitis (changes may persist to
some degree after acute exacerbation)
Muscle pain, "acid feeling":
1: slight pain, acid feeling develops after moderate exercise,
requires hours rest
2: moderate pain, acid feeling ved slight exercise (ex. sore
leg muscles after <500 meter walking distance), requires days
rest
3: severe pain, tired, sore, acid feeling all the time without exercise,
not relieved by rest for days
Muscles - cramps, fasciculations, twitching, tremor, wobbling, clonus,
jerks:
1: feeling of slight movement, not objective / not visible by
others
2: objective tremor, fasciculation, jerks
3: clonic/tonic cramps (- remember to describe level of conciousness
during attack and duration in PT-notes)
Muscle weakness, paresis, drop attack:
1: feeling reduced force, but not objectively reduced
drop-attack: a sudden involuntary
unexpected loss of muscle tone when in legs leading to a fall (or in
hands dropping things), without loss of conciousness, that is over in
seconds or a few minutes
- describe in PT-note
2: paresis, objectively reduced force, but the muscle / limb can be
moved by the patient
3: paralysis, limb can not be moved by muscle force
Morning stiffness (joint, muscle):
[0: no]
1: yes
- describe where and how long and what helps in PT notes
Bone pain:
- is usually deep, penetrating, or dull.
1: slight, few stabbing pains of short duration (seconds)
2: moderate, pain lasts minutes to hours
3: severe pain, present all the time
Skin:
Skin pain:
- burning, stabbing - describe type and location in PT-notes
1: slight but short lasting (minutes) burning pain after
touch
2: moderate burning, longer lasting than normal (hours) after even a
slight touch, that should not hurt normally
3: severe burning (like a severe sunburn) present all the
time
Reduced sensibility:
- prickling, numbness - describe location in PT-notes
1: slightly reduced - slight numbness and prickling, but can sense
touch (that may elicit burning)
2: moderately reduced - numbness and prickling, reduced sense of warm
and cold touch, reduced sensibility for needle prick
3: severe numbness, can't feel anything on touch
Itching:
- describe localisation in PT-notes
1: slight itch, can abstain from scratching
2: moderate itch, disturbing, need to scratch
3: severe itch, all the time, very disturbing, can't sleep for it,
scratching marks on skin, if long term may lead to leathery thickening
(lichenification)
Rash (non-hemorrhagic) or sores:
[0: no]
1: yes
- describe localisation, appearance/color, size and duration TAKE PHOTO
(with ruler besides) when possible
Hemorrhagic rashes:
- describe localisation, appearance/color, size, consistency (if felt)
and duration - TAKE PHOTO (with ruler besides) when possible
1: few and tiny, (pinpoint petecchiae), occurs mainly after scratching
or pressure applied to the skin
2: a lot, small mm size spots (vasculitis like) to larger (more cm)
sugillations, occurs spontaneoulsy on arms and legs especially
declive, but rarely on truncus
3: many spontaneusly ocurring bleeding spots of various size, overall
but mostly extremities
Brain, Neurological symptoms:
Headache:
- describe localisation in PT-notes
1: slight - mental function reduced, but possible to "pull yourself
together", physical strain makes headache worse
2: moderate - can't think or work, must rest - but able to be
up and can eat
3: severe - migraine like - can't do anything, bedridden - headache
usually accompagnied by other "neurotoxin" symptoms like light- and
sound sensibility, nausea, sometimes vomiting
Shooting pain / lightning / stabbing pain:
- describe localisation in PT-notes
1: a few times a day
2: once per hour
3: several times per hour
Brainfog / like being in a glass case:
"Brainfog may be described as a state of confusion or lack of
clarity. It can feel like a cloud that reduces your visibility or
clarity of mind. It can cause you to become forgetful, detached
and often discouraged
and depressed."
1: can't concentrate on following conversation if something else distracting is going
on nearby, like when many others are talking, background noise (get foggy at party, in a shopping mall)
2: can't concentrate on following conversation, even when quite and only one person is
talking to you at a time
3: do not understand anything, feel like being in another world /
outside oneself / spectator to a silent movie; 'flickering
on TV' the meaning do not pass into the brain / is not
perceived
Disorientation / getting lost, going to wrong places:
1: slight problems finding way in unknown plaves, but can understand and follow directions
2: moderate problems finding way in known places, problem finding out which direction one is going
3: gets lost even in wellknown places, enters the neighbors door instead of ones own door
Concentration difficulty:
1: slight problems sticking the mind to try solve a difficult task
(work), but can do relaxing things like watching
entertainment in TV, read magazine
2: moderate - can concentrate on easy things like entertainment in
TV, but can't concentrate on reading a book nor follow the plot in a
detective story; can't stick to solve a task, but is easily distracted
by interruptions and can't pick up and continue with solving the task
after the break
3: severe - can't concentrate on anything, even not light entertainment
/ comedy, can't read and understand even a few lines of text in a
magazine
Memory problems (usually short term):
1: need help from writing notes, calendar, alarms to remember
appointments and have "post-it" everywhere, in order to remember what
to do, remember to buy etc. - but with these aids can function
pretty normally (i.e. others may not notice you have memory problems);
you have no problems remembering your PIN codes to different credit
cards or your familys and friends phone numbers that was learned
before, but can have much trouble learning new numbers
2: can't keep track of anything without notes (but forget to look in
them), forgets wellknown routine things link PIN and phonenumbers, if
going for something but comes back without, several times … i.e. all
tasks are done slow, bad and usually with many repeated trials before
success (your credit card may get closed because you continue entering
wrong PIN numbers).
3: can't tell what you was told 5 minutes ago, have difficulty
remembering how to do common tasks, maybe can't remember what your own
notes mean, i.e. unable to do activities of normal daily living, thus
need help from others
Difficulty with finding words / spelling / word search / name block:
1: slight problems - make letter / numbers reversals, but
notice and correct during proof-reading, no problems with forming
sentenses or finding words
2: moderate problems ....
3: severe problems finding words (may try forming new words as
replacement), sentences backwards, many letter reversals /
spelling errors, which is not found despite more proofreadings ..
Perception / comprehension / ability to understand meaning of what is written / said:
1: slight problems - can understand simple messages, but have problems grasping the meaning of more complex explanations
2: moderate problems ....
3: severe problems - can not understand even simpler messages
Dizziness / poor balance:
1: slight - dizzy spells / sense of nearly fainting - of few minutes duration and only a few timer during 24 hours
2: moderate - feeling drunk / intoxicated / dizzy spells comes several times a day and/or lasts for hours
3: severe vertigo - feeling like the room is spinning around or like the floor is moving up and down under your feet
Psyche:
Low self esteem:
[0: I'm okay and believe in myself]
1: slight - I realize there are things I can not do anymore, but the
illness gives a natural explanation for why, and no matter what
others say, I know the cause of my problems is not
a mental illness.
2: moderate - there are many things I can not do, others are partially right when they say it is psychic
3: severe - I am no good at anything, others are always better and always right, I believe them when they say I'm depressed
Mood swings - cyring spells:
[0: no]
1: yes - describe the situation in PT-notes
Suicide thoughts:
[0: never had]
1: slight - rarely and can be talked out of it / can alter my negative
thoughts by intentionally thinking positive, thinking "what could be
worse"
2: moderate ....
3: severe - thinking life is way too difficult to live on, as it is now, have thought on how to commit suicide
Irritability, lack of impulse control, "short fuse":
1: slight - 'short fuse' and feeling irritable within, but without leading to uncontrolled, unsuitable actions
2: moderate - you have temper tantrums, scream at others, but can stop yourself before violence or destruction
3: severe - lack of impulse control, leading to uncontrolled, unacceptable actions, like violence or destruction
Anxiety:
1: slight - only occasional fear which can be controlled
2: moderate - fight hampers functions out of home, but you manage quite well at home
3: severe - anxiety / fear hampers all functions, everywhere
Sexuel function - desire/libido, ability:
- describe in PT-note
1: slightly abnormal - increased desire and able to perform normally
2: moderately decreased libido, but can perform coitus
3:
severely decreased libido / ability, can not perform coitus